[QUOTE="Kimmyt, post: 332822, member: 89"
I'm not sure I actually agree with this. Perhaps this would be true if the pelvis and hips moved independantly of the rest of the body, but that is not what happens. When the hips are out of neutral, the rest of the skeleton/body adjusts. This is why we have certain postural patterns that go along with anteriorly tilted pelvis (forward head position, rounded shoulders etc). So, if someone has an anteriorly tilted pelvis while skiing, because of the compensations one has to make in other parts of the body due to the tilted pelvis, it can be much harder to balance while achieving matching angles.
Basically, my main point is that you can't ignore pelvic tilt when considering stance because when the pelvis is shifted out of neutral (anterior or posterior), 1) the muscles do not work to full efficiency and 2) the skeleton is positioned in such a way that full rom (which is a function of the muscles ability to move as they are intended) is impossible or at the very least hard to achieve. Of course, it's very true that if a person struggles with these issues that corrective exercise out of skiing lessons is probably more beneficial, but it's worth bringing their attention to it because many people are unaware of pelvic tilt.[/QUOTE]
"Reactive Lumbo-Pelvic Control Program
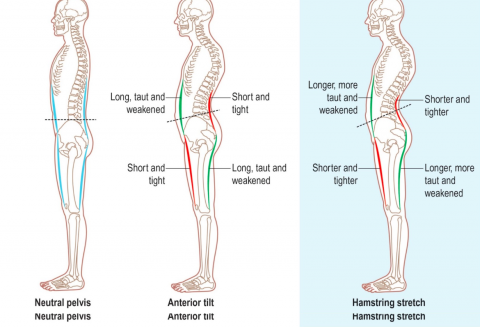
One of the most common postural dysfunctions seen is the anterior tilted pelvis associated with an increased lordosis. A list of compensations and adaptations such as thoracic kyphosis, hyper-extending knees, hamstring over activity, abdominal insufficiency, mechanical low back pain, etc. are often then attributed to the central postural dysfunction of the pelvic tilt.
However, it is probably quite unfair to blame the pelvis for this “chain” of dysfunction as its position is generally dictated by the length, tension and activity of the structures that surround it. It is merely being pulled into this shape, and its position can be a structural “symptom” of the muscle imbalances, fascial shortening and adaptations that are present.
" Common techniques used in reactive motor training are to
position the body or use resistance forces
that, if overcome automatically,
recruit our target muscle groups and facilitate postural positional change... in this case, a stable pelvis with a more neutral/level tilt"
"Lower Extremity Injury Prevention"
References:
- Clark, Mike. Essentials of Integrated Training Series. 2001-2003
- Cook, Gray. Functional Movement Screening Exercise Progressions. 2005
- Cook, Gray. Athletic Body in Balance. Human Kinetics, 2003
- Norris, C. Back Stability. Human Kinetics, 2000
- Page, Phil. The Janda Approach to Musculoskeletal Pain.
The matching angles is also called figure-4 position in corrective exercise or functional movement training in which the verbatim objective is: " To promote optimal alignment between the trunk and tibia, as well as optimal position of the spine". This position helps to neutralize the spine by optimizing gluteal activity and inhibiting quad dominance. The problem with moving into the backseat from this position is more than likely : using the knees instead of hips to achieve the position which reverts back to quad dominance, lack of dorsi -flexion or locking the ankle into a fixed position as indicated in the video. The importance of this being, the ankle and glutes are bed partners - when the ankle is locked the glute rolls over and goes to sleep - when the ankle moves back and forth the glutes are turned on. Sleeping glute = quad dominance, back seat, anterior pelvic tilt. Turned on glute = neutral spine, stable position. This guy is doing a front squat so his shift is somewhat different but the point remains the same.